Amino Acids for Super Humans, Part IV - Purported Ergogenics (2/3): L-Carnitine, ALCAR, LCLT, GPLC & Co.
 |
| Image 1: Even bought in bulk, the carnitines are not exactly cheap, so you better read on to gather whether ALCAR, L-CAR, P-LCAR, L-CLT & Co are worth spending money on. |
Necessary co-factors for carnitine synthesis are
- ascorbic acid (vitamin C),
- pyridoxine (vitamin B6),
- niacin (vitamin B3) and
- S-Adenosyl methionine (SAMe)
 |
| Note: This is the detailed transcript of my show notes to "Amino Acids for Super Humans Part IV" click here to download the podcast if you want to listen before / during / after you read the rest of the notes |
Did you know? The first soy-based baby formulas were low in carnitine, so that neonates who were fed respective products had 1/3 lower carnitine levels than babies who were breast-fed or received milk-based products. Even in the absence of symptoms of overt carnitine deficiency, sub-optimal carnitine levels put these children at risk of early or late metabolic complications (Olson. 1989). Consequently, almost all soy-based infant formulas are enriched with l-cartinine, today.
Vegetarians and Vegans generally have lower plasma carnitine levels
 |
| Table 1: Amount of carnitine in food; meat, fish and dairy are particularly good sources of dietary l-carnitine (data adapted from wikipedia.org) |
That's unfortunate news for all vegetarians and vegans out there, because as the data in table 1 shows, meat, fish and dairy are the richest dietary sources of l-carnitine. "Omnivorous humans generally ingest 2-12 µmol of carnitine per day per kg of body weight" (Vaz. 2002), which is up to 10x the estimated amount of our endegenous production (1.2µmol /kg/day). So that 75% of the well-stocked carnitine stores of meat-eaters come from dietary, and only 25% from de novo biosynthesis. Needless to say that, with an average daily carnitine intake of <0.1µmol /kg body weight, vegetarians and vegans are usually significantly lower than those of their omnivores fellow men (Rebouche. 1992).
Symptoms of overt carnitine deficiency, such as cardiomyopathy,
hepatomegaly, myopathy, recurrent episodes of hypoketotic
hypoglycaemia, hyperammonaemia and failure to thrive have yet not been observed in the absence of CDSP (primary carnitine defiency), a pathology that has been mapped to human chromosome 5q and is characterized by excessive renal and intestinal wastage of carnitine.
Attention Atkins dieters! In a German study (Liebhaber. 2006) the long-term effects of ketogenic diets on epileptic children, carnitine deficiency was detected in 57% of the patients who did not receive supplemental l-carnitine. There was a large interpersonal variety as far as the onset of carnitine deficiency was concerned. On average subjects developed carnitine defiencey after about 32 weeks, one subject was however carnitine deficient after only two days and one subject maintain sufficient carnitine levels for 248 weeks before carnitine deficiency was diagnosed. These observations stand in line with results of Stadler et al. (Stadler. 1999) who had previously established that a high fat intake increases carnitine excretion. Taken together, this data suggests that people who follow a high fat (not the high protein low carb diet everybody is on these days) would generally benefit from carnitine supplementation.
How carnitine facilitates "fat-burning"
 |
| Illustration 1: Carnitine is like the man who shovels the coal. It's just a small wheel in the mitochondrial fat burning machinery. Without lipolytic activity (= free fatty acids floating aroun) and a sufficient number of properly functioning mitochondria, increased carnitine levels won't translate into fat loss (picture in the back- ground from Ptak Science Books. 2009) |
The commonly touted "fat burning" effects of l-carnitine (and all other forms of carnitine) thusly belong to the realms of advertismental oversimplifications, or should I say frauds? Even taken poundwise carnitine by itself will neither empty, nor burn the contents of a single of your unaesthetic fat cells. On the other hand, a profoundly lowered carnitine levels as they were reported for elderly and obese patients by Noland et al. (Noland. 2009) could lead to or exasperate existing weight problems by compromising the transport of fatty acids from the cytosol, i.e. the intracellular fluid, into and back out of the mitochondria.
 |
| Figure 1: Free and bound (esterified) carnitine content in mg/kg of different meat products (data adapted from Seline. 2007) |
In and out that's the way things have to go
 |
| Image 2: Lipofuscin accumulation (fine brown / yellow granular pigment) in liver cells (photo by Nephron). |
Inter-cellularly, carnitine also functions as a temporary buffer for the unused acetyl-CoA. The accumulation of respective acyl-carnitines within the mitochondrion, which goes hand in hand with a depletion of unbound l-carnitine that would faciliate the transport of fatty acids into the mitochondria, has been implicated as one of the confounding factors in the etiology of the metabolic syndrome.
 |
| Figure 2: Simplified illustration of the underlying mechanism of carnitine mediated fatty acid transport in and out of the mitochondrion (The AOCS Lipid Library) |
L-Carnitine as a selective glucocorticoid receptor modulator & useful tool in hyperthyroidism
Beside its effects on mitochondrial health, l-carnitine also exhibits anti-inflammatory properties by directly interacting with glucocorticoid receptors on immune cells (Manoli. 2006). In experiments Manoli et al. conducted back in 2006, l-carnitine in a glucocorticoid-like fashion "suppressed the lipopolysaccharide-stimulated release of tumor necrosis factor α and interleukin-12 from primary human monocytes". Despite its ability to stimulate glucocorticoid receptors (GR), and to reduce binding of the cortisol analogue 3H]-dexamethasone to GRs, LCAR apparently lacks the deleterious side effects corticosteroids have on other organs/tissues in the human body.
Moreover, a study by Benvenga et al. in which women received supraphysiological doses of the synthetic thyroid hormone levothyroxin (T4) to induce symptoms of hyperthyroidism confirmed previous observations that l-carnitine even at doses as low as 2-4g/day "antagonizes hyperthyroidism-related [...] symptoms and biochemical responses of thyroid hormone target tissues". Data from cell culture experiments suggest that it is the property to inhibit T3 and T4 entry into cell nuclei, which it at the heart of the anti-(hyper-)thyroid effect of l-carnitine, since l-carnitine supplementation does not substantially affect thyroid hormone levels or radioactive iodine uptake by the thyroid.
Did you know? Both full-blown hyper- as well as hypothyroidism have been associated with muscular carnitine depletion (Sinclair. 2005), as a consequence of insufficient synthesis (hypo-) and increased usage (hyper-) of carnitine.
In that, it is interesting to note that, vice-versa, thyroid hormone also influences the rate of carnitine synthesis (Galland. 2002), which, again, brings up the idea of tightly regulated, feedback-control mechanisms intended to keep the metabolic rate (including the mitochondrial beta oxidation of fatty acids) in a narrow physiological range, so that in people with high levels of thyroid hormones (not necessarily hyperthyroidism) and increased carnitine production, or in people with low levels of thyroid hormones (not necessarily hypothyroidism) and decreased carnitine production the respective ratios of carnitine / thyroid hormone could lead to similar cellular T3 / T4 uptake in the presence of fundamentally different serum levels of these hormones.Carnitine intake and clearance - does supplementation make sense at all?
In healthy human beings, on the other hand, the main regulatory mechanisms take place in the kidney and a basic understanding of the relation of carnitine intake to urinary loss is of fundamental importance for anyone who does not want to feed his expensive carnitine supplements to sewer rats.
 |
| Figure 2: Free and bound (esterified) carnitine content in mg/kg of different milk products (data adapted from Seline. 2007) |
In general, dietary l-carnitine has a bioavailability of 54%-84% and is thusly much better absorbed than supplemental carnitine in powdered or capped form, for which Rebouche et al. report a bioavailability of meager 14%-18% (Rebouche. 2006). Ideally, you would thus get about 1.28g of carnitine from 1kg of Kangaroo steak, which turns out to be by far the best source of dietary l-carnitine.
Note: According to the data from Rebouche et al. you wanted to get the same 1.28g of carnitine from a supplement, instead of a 3-4 dilicious steaks, you would have to consume 7-9g of supplemental carnitine in pill or capsules for the same amount of l-carnitine to hit your blood stream!
A vegan, who abstains from eating meat, fish and dairy, on the other hand, would have to eat his share of 60kg of mushrooms to get an equal amount of 1.28g of carnitine. Although the act of eating 60kg of mushrooms would already border the supernatural, the of 320kg of carrots you would have to eat, alternatively, are merely hypothetical. |
| Figure 3: Free and bound (esterified) carnitine content in mg/kg of different mushroom, vegetable and fruit products (data adapted from Seline. 2007) |
 |
| Figure 4: Total ingested (full bars) and absorbed (blue part of the bar) amount of dietary carnitine in mg/kg body weight (data adapted from Rebouche. 1999 & Rebouche. 2006) |
Did you know that multiple small doses of carnitine are way superior to a single large dose if your aim is to persistently increase serum carnitine levels? In contrast to Rebouche et al. (Rebouche. 2006), who achieved relatively stable carnitine levels >50% above baseline by having their subjects take their 2g of carnitine in three divided doses (at 8am, 12pm, and 6pm) trials using a single, large bolus of l-carnitine (orally and even intraveniously) did not produce sustainable elevations in plasma carnitine levels. Furthermore, the addition of carbohydrate (96g glucose in addition to 3g l-carnitine/day) and the concomitant insulin release have been found to decrease uriniry carnitine clearance, or, converesely, increase carnitine retention by ~40% (Stephens. 2007).
The decreased absorption of dietary carnitine from the gut goes hand in hand with a decreased reabsorption of carnitine in the kidneys. At low to normal serum carnitine levels the latter conserve 90-99% of the circulating carnitine. When carnitine levels increase, however, the clearance rate increases way beyond the 1-3 mL/min that would leave your body in the form of urinary losses under "normal" circumstances. Thusly, increased carnitine levels, as they are the result of an intravenous infusion of 0.5g of carnitine, return to baseline in less than 12h, with a rapid decline (-80%) in the first hour after administration. Whole body turnover, i.e. the "renewal" of creatine stores, in slow (muscle) and fast turnover (liver, kidney, and other tissues) stores is estimated to take about 38-119h (Rebouche. 2006).On the different forms of carnitine
The absorption issue immediately reminds me of the bro-scientific mambo-jambo about the bioavailability of different forms of carnitine you can find wherever L-CAR, ALCAR, P-LCAR, LCLT & Co are sold. In most cases the the individual bioavailibility appears to depend on the venue the respective vendor will get from the different forms of carnitine. In that, supplement manufacturers cash in on the lack of scientific studies comparing the absorption kinetics of the various commercially available forms of carnitine in a single objective model. In this context it is also noteworthy that both commercially available carnitine-esters, i.e. acetyl-l-carnitine (ALCAR) and (glycine-)propionyl-l-carnitine (PLCAR, (G)PLC), are no invention of the supplement industry, but naturally occurring forms of carnitine, the pharmacokinetics of which have been studies by Cao et al. after oral administration of 2g of l-carnitine to 12 healthy volunteers (Cao. 2009).
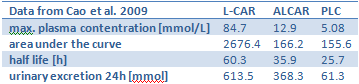 |
| Table 2: Pharmacokinetics of l-carnitine (L-CAR), acetyl-l-carnitine (ALCAR) and propionyl-l-carnitine (PLC) after oral administration of 2g of l-carnitine to 12 healthy volunteers (data adapted from Cao. 2009) |
The results of Cao et al. stand in line with findings of Eder et al. (Eder. 2005), who used a pig model ( which is pretty reliable when it comes to modeling the human digestive system) to estimate the bioavailability of various L-carnitine esters (acetyl-L-carnitine and lauroyl-L-carnitine) and salts (L-carnitine L-tartrate, L-carnitine fumarate, L-carnitine magnesium citrate) and found that
AUC [aera under the curve] values, calculated for the time interval between 0 and 32 hours, for both free and total carnitine were similar for base of free L-carnitine and the three L-carnitine salts (L-carnitine L-tartrate, L-carnitine fumarate, L-carnitine magnesium citrate) while those of the two esters (acetyl-L-carnitine, lauroyl-L-carnitine) were lower.In that, it is of particular interest that l-carnitine-l-tartrate (LCLT), which is heavily promoted as the "best" carnitine supplement, did in fact "yield a higher plasma free carnitine AUC value for the time interval between 0 and 3.5 hours than [any] of the other compounds." The faster absorption of LCLT aside, the data of this (unfortunately) unique study would suggest that the fancy "L-carnitine salts have a similar bioavailability" as the way cheaper free form of carnitine (l-carnitine) and both appear to be better absorbed than any of the l-carnitine esters .
Did you know? Gram per gram the tartrate salt of carnitine (LCLT) provides only 40% carnitine. If, for example, you wanted 2g of pure carnitine, you would have to take 5g of LCLT.
Acetyl l-carnitine the one and only (?) brain booster
In the case of ALCAR, for example, it is well established that its oral bioavailability is decreased due to increased hydrolysis. Oral bioavailability, on the other hand, is only one of the attributes the addition of the acetyl ester to the free form of carnitine changes. For example, it is often cited that ALCAR would be the only form of carnitine that is able to pass the blood-brain-barrier (BBB) in mammals. This statement is simply false! While it is true that the acetylated form of carnitine passes enters the brain more easily, i.e. it takes lower concentrations outside the barrier to achieve the same levels of carnitine within the brain, the difference in K(m) values, which area a measure of the concentration of substrate required to produce 50% of the maximal uptake, is only 5% (K(m)Alcar=31.3 vs. K(m)Carn=33.1, cf. Kido. 2008).
Anyway, at least those of you who have some sort of cognitive / neurological problem, probably won't really care if ALCAR is actually the only, or maybe just the favorable form of carnitine to treat neurological diseases, as long as it will help mitigate your problems - and indeed, ALCAR appears to be a formidable "brain nutrient" which has been used succesfully in a variety of brain-related clinical conditions (Alternative Medicine Review. 2010):
- Alzheimer's disease
- Depression
- Attention deficit / hyperactivity disorder (ADHD) and Fragile X Syndrome
- Peripheral (diabetic, antiretroviral and chemotherapy-induced) neuropathy
- Cerebral ischemia and reperfusion
- and others
- Increasing neural energy production
- Protecting neurons from toxins
- Maintaining neuron receptors
- Increasing availability of the neurotransmitter acetylcholine
- Decreasing accumulation "damaged fats" (lipofuscins) in brain tissue
 |
| Image 3: Molecular structure of the bulky 3-Propanoyloxy- 4-(trimethylazaniumyl)butanoate molecule which usually goes by the name Propionyl-L-carnitine, or its abbreviations PLC or PLCAR. |
Note: I assume, you have also heard of the paradoxical effect 4.5g of GPLC had on sprint performance in a 2010 follow-up study of Jacobs et al. (Jacobs. 2010). In contrast to what the scientists had expected based on previous results (Jacobs. 2009), long-term supplementation of a high dose (4.5g vs. 1.5g) of glycine propionyl l-carnitine did not only fail to improve sprint performance beyond what was achieved with 1/3 of the dosage, the huge pump, the athletes were complaining about, even compromised their performance. If you are an athlete, exceeding a dose 1-2g of GPLC per day would thus be more than a waste of money, it could actually cost you your victory. Remember: With most supplements taking more does not equal greater benefits!
L-carnitine l-tartrate the one an only (?) testosterone booster |
| Image 4: "Supported" studies make LCLT highly marketable (Lonza, Inc) |
Did you ever think of the remote possibility that the "subtle yet significant" effects l-carnitine l-tartrate had on androgen receptor expression and testosterone in the heavily cited 2006 study by Kraemer et al. (Kraemer. 2006), may come from the tartrate and not the carnitine? Me neither, but the idea Owner (pseudonym) from the Mind&Muscle boards brought up, back in the days, is not totally devious. Join the smartest BB-community on the net and revive the discussion, if you will!
Conclusion
Do you remember? This write-up started out with the purported fat-burning effects of carnitine, established that carnitine is a necessary, but not sufficient co-factor in mitochondrial beta oxidation and clearance of fatty acid, elaborated on the metabolic and neurological health benefits of carnitine and concluded on the true ergogenic value of what turned out to be a whole group of quite expensive amino acids, the use of which you should take into consideration only after you got your (carnivorous) diet, your training regimen and your basic supplement protocol (protein, creatine + facultative EAA/BCAA) in check.


